A NEW YEAR, NEW HOPE IN THE FIGHT AGAINST HIV WITH LENACAPAVIR —NO CAP!
By: Adhella Menur
As a member of the INA-RESPOND Science team, I am thrilled with the acceptance of the first publication from our HIV study, entitled “A Prospective Observational Cohort Study of HIV Infection in Indonesia: Baseline Characteristics and One-Year Mortality” in the BMC Infectious Dis-eases journal. This paper provides valuable evidence for Indonesia and serves as a foundational reference for future exploratory publications. Reading the paper, it becomes evident that the chain of HIV infection in Indonesia remains far from being broken. The most commonly observed modes of HIV transmission were high-risk sexual activities, including heterosexual and men who have sex with men (MSM), as well as intravenous drug use (IDU). Alarmingly, more than half of the participants were late presenters, meaning they were diagnosed with HIV only after reaching WHO clinical stages III or IV. One year into the observation, we found that the UNAIDS target of 95% viral suppression was not achieved, even though the study was mostly conducted at major referral hospitals in large cities. This highlights significant gaps in early detection, treatment challenges, and outcomes, ultimately resulting in a high risk of ongoing transmission within communities. A re-cent statement from the Ministry of Health revealed a continuous annual increase in new HIV cases, with the highest prevalence among productive age groups (25–49 years).
Having said that, there is an urgent need for enhanced prevention strategies to curb the HIV epi-demic. While HIV vaccines are still under development, optimizing the use of highly efficient and effective Pre-exposure Prophylaxis (PrEP) is critical. At the end of 2024, the journal Science named Lenacapavir the Breakthrough of the Year, rec-ognizing its remarkable results as a PrEP option with 96–100% efficacy. Science described it as “a pivotal step toward diminishing HIV/ AIDS as a global health crisis. In this New Year edition, we will explore how Lenacapavir offers new hope to break the chain of HIV transmission—No Cap!
Lenacapavir: the first-in-class, long-acting, multistage capsid inhibitor
Lenacapavir describes how basic science research lays the groundwork for translation into clinical practice. Dr. Wesley Sundquist, a Samuels Professor and chair of biochemistry at the University of Utah, along with his team, dedicated their re-search to understanding the molecular structure of HIV and its mechanisms for infection and replication. Sundquist’s team focused specifically on the HIV capsid protein (p24), a cone structure that encapsulates HIV RNA. This capsid protects the viral RNA and facilitates its transport into the host’s nucleus. In fact, the capsid does not immediately fall apart when HIV enters a cell, as previously thought, but remains intact and can even squish through pores in the nuclear membrane to deliver its payload of viral genes. The capsid plays essential roles throughout the HIV replication cycle, and Sundquist’s team figured out that disrupting this structure could prevent the virus from assembling properly or entering host cells’ nuclei.
These groundbreaking insights inspired the pharmaceutical company Gilead Sciences to explore the development of drugs targeting the HIV capsid, with Sundquist as the consultant.
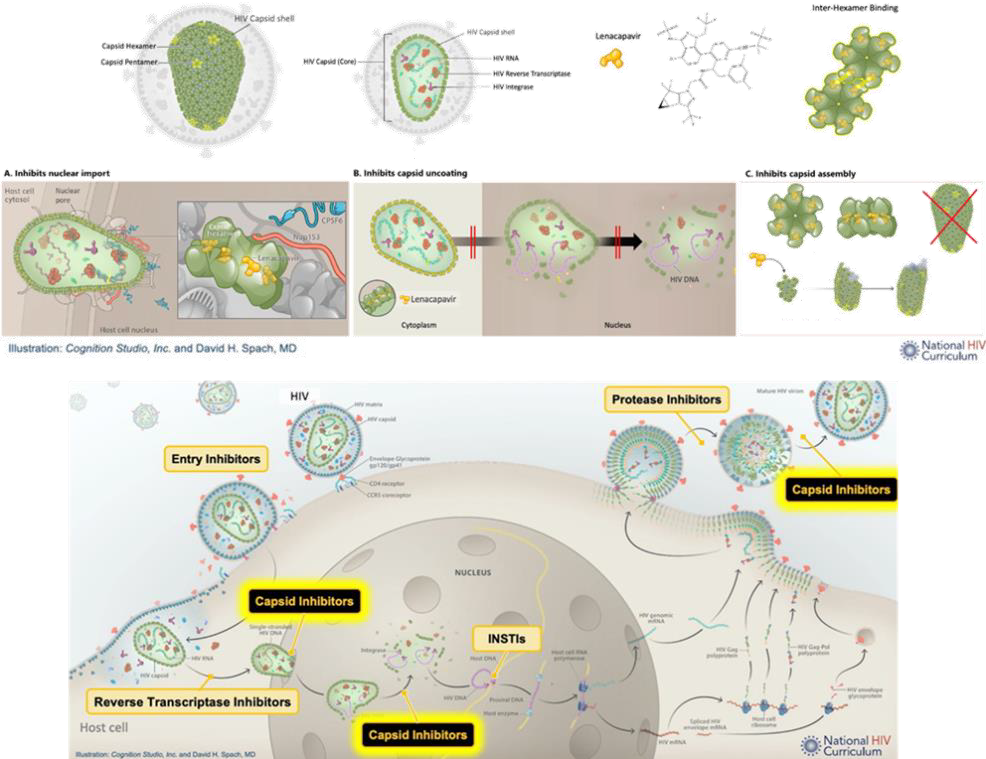
With the benefit of X-ray crystallography, the team designed Lenacapavir (initially known as GS-6207), which targets a highly conserved capsid interface and exerts multistage, selective inhibition of the HIV capsid. By interfering with capsid-mediated nuclear uptake of pre-integration complexes and impairing virion production, Lenacapavir inhibits viral replication at both early and late stages of the life cycle:
- Inhibits nuclear import: By making the capsid cone rigid, Lenacapavir prevents it from slipping into the nucleus. Additionally, it binds to the same capsid interface utilized by host nu-clear import co-factors, such as nucleoporin 153 (Nup153) and cleavage and polyadenylation specificity factor 6 (CPSF6), thereby interfering with the transport of viral complexes to the host nucleus.
- Inhibits capsid uncoating: Lenacapavir stabilizes the capsid shell, preventing its uncoating and thereby halting viral replication during the initial stages of infection.
- Inhibits capsid assembly: Lenacapavir disrupts the capsid lattice during the maturation phase of the virus, rendering newly formed HIV particles non-infectious.
In the development of Lenacapavir, the team also highlighted the importance of a long-acting agent to improve adherence and ensure successful intervention. To maintain effective plasma trough concentrations over an extended period, a long-acting drug must exhibit high potency, a slow and sustained release rate, and a slow systemic elimination rate. Following oral administration, Lenacapavir is unaffected by food intake, has a half-life (t1/2) of 10–12 days, and has an apparent clearance of 55 L/h. With subcutaneous (SC) administration in the abdomen, it demonstrates a significantly longer t1/2 of 8–12 weeks and a lower ap-parent clearance of 4.2 L/h. A slow initial rise in plasma levels was observed during the first few weeks following SC administration, which led to the consideration of an initial pharmacokinetic loading dose using oral Lenacapavir. The primary route of excretion is through feces, accounting for 76% of all excreted drug, with 33% excreted un-changed, while less than 1% of the drug is eliminated renally. Lenacapavir is thus characterized by low human clearance and low aqueous solubility, which supports its administration every 6 months. The FDA emphasized that the optimal dosing interval is 26 weeks to ensure plasma trough concentrations consistently remain above the minimum drug concentration required to inhibit the virus effectively.
With its novel mechanism of action, Lenacapavir has no overlapping resistance with any approved agents, and no preexisting resistance or polymorphisms have been identified that reduce viral susceptibility to the drug. However, emergent resistance to Lenacapavir was observed in clinical studies, although it was often associated with a high fitness cost to the virus. This indicates that while resistance may develop, it comes at a significant disadvantage to the virus’s ability to replicate and survive. Further observation and monitoring are unquestionably needed to fully understand and manage the potential for resistance.
Lenacapavir was approved by the FDA on December 22, 2022, for the treatment of heavily treatment-experienced adults whose current antiretroviral therapy (ART) regimens were failing due to resistance, intolerance, or other safety concerns. The approval was based on results from the Phase 2/3 CAPELLA trial, which evaluated the efficacy and safety of Lenacapavir in combination with an optimized background regimen for patients with multidrug-resistant HIV-1 infection.
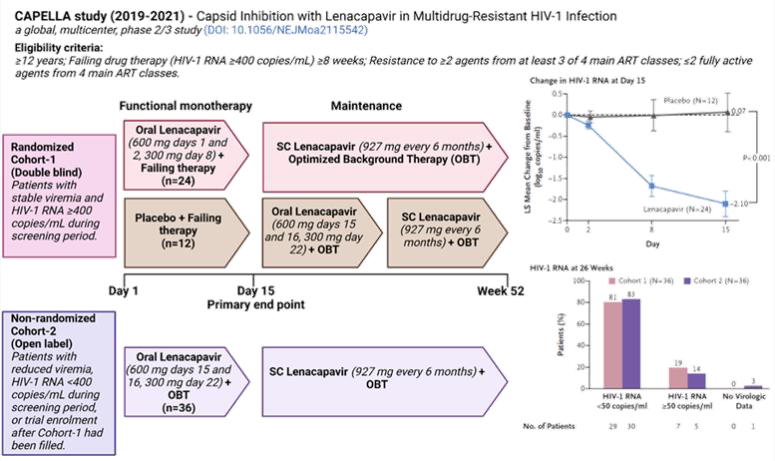
Lenacapavir demonstrated significant efficacy as functional monotherapy, leading to a substantial decrease in viral load. When combined with optimized background therapy, Lenacapavir achieved high rates of virologic suppression and a clinically meaningful increase in CD4+ counts. During the maintenance period, Lenacapavir-associated cap-sid mutations were observed in 8 patients (4 in Cohort-1 and 4 in Cohort-2). Among these, 6 patients exhibited an M66I mutation (including one with M66I + N74D), while other mutations included Q67H + K70R and K70H. Despite these mutations, some patients maintained viral load sup-pression while continuing Lenacapavir with minimal or no adjustments to their optimized back-ground therapy.
No serious adverse events related to Lenacapavir were reported. Most adverse events were mild or moderate, with the most common being injection-site reactions. The SC administration of Lenacapavir every 6 months eliminates the need for daily pills, maintaining therapeutic drug levels between visits. This long-acting regimen reduces the uncertainty and variability associated with incomplete adherence, offering a significant advantage for patients.
The PURPOSE-1 & PURPOSE-2 Studies: Groundbreaking evidence supporting Lenacapavir’s role in HIV Prevention
PrEP is an amenable strategy to achieve the ambitious UNAIDS target of Zero new HIV infections by 2030. Numerous clinical trials have validated the efficacy and safety of PrEP; however, its success is heavily reliant on adherence, which remains a sig-nificant challenge as it requires individuals to make positive health choices consistently. Poor uptake and adherence to daily pill regimens weaken PrEP’s effectiveness. To address this, several approaches such as the monthly Dapivirine vaginal ring, bi-monthly intramuscular injections of Cabotegravir, and intravenous infusions of broadly neutralizing antibodies (VRC01) every 8 weeks have been explored. Adding to these strategies, twice-yearly SC injection of Lenacapavir emerges as a promising solution to improve adherence and ensure effective PrEP. “It has the potential, if we can do it right, which means going big and getting it out there,” says Professor Linda-Gail Bekker, an infectious disease specialist at the University of Cape Town who led PURPOSE-1 study, one of the two Lenacapavir efficacy trials.
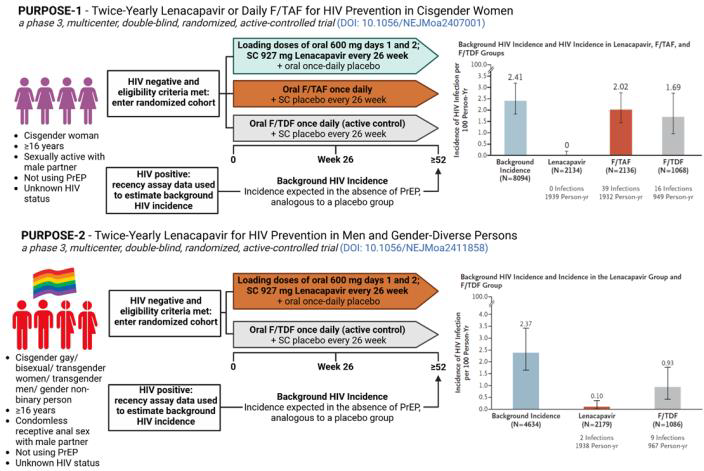
(Source: Bekker LG et al., 2024, DOI: 10.1056/NEJMoa2407001; Kelley CF et al., 2024, DOI: 10.1056/NEJMoa2411858). F/TDF: emtricita-bine–tenofovir disoproxil fumarate; F/TAF: emtricitabine–tenofovir ala-fenamide; cisgender: a gender iden-tity that corresponds to their sex assigned at birth; gay: sexually at-tracted to people of the same sex or gender; bisexual: sexually attracted to more than one sex or gender; transgender: a gender identity that does not correspond with the sex registered for them at birth; gender non-binary: a gender identity that is not exclusively male or female. Cre-ated with Biorender.com.
The PURPOSE-1 study of Lenacapavir delivered astonishing results as HIV PrEP, demonstrating 100% efficacy among adolescent girls and young women in South Africa and Uganda. This was fol-lowed by the PURPOSE-2 study results, which showed 96% efficacy among gender-diverse per-sons who have sex with men in the United States, South Africa, Peru, Brazil, Argentina, Mexico, and Thailand. During the PURPOSE-1 study, there were 193 pregnancies in the Lenacapavir group, with no HIV infections reported. A congenital abnormality, polydactyly, was observed in an infant born to a participant in the Lenacapavir group. However, the investigator determined this abnormality to be unrelated to the drug, as the participant had a strong family history of the condition. In the PUR-POSE-2 study, two cases of HIV infection were reported in the Lenacapavir group during the trial period, both associated with the emergence of capsid resistance (N74D mutation) resulting from Lenacapavir monotherapy. While cases of HIV infection despite PrEP use have been documented—often linked to high exposure levels and repeated mucosal injury—more than 99% of participants in the Lenacapavir group remained free from HIV infection, even amidst high levels of sexual expo-sure, drug use during sex (‘chemsex’), and sexually transmitted infections. Poor adherence to daily oral F/TAF or F/TDF observed in these studies may be attributed to various factors, including stigma, dislike or lack of experience with daily pill-taking, and misconceptions about the risk of acquiring HIV infection.
Lenacapvir, a twice-yearly PrEP option, presents an opportunity to address challenges of adherence and persistence, offering substantial protection against HIV infection for diverse populations. According to Gilead Sciences, data from the two trials will be used to support a series of global regulatory filings starting by the end of 2024. The aim is to launch Lenacapavir onto the market in 2025.
Looking ahead: Challenges and hopes
Lenacapavir, the Breakthrough of the Year 2024, brings new and powerful hope in the fight against the HIV epidemic. However, to unleash its full po-tential for both HIV treatment and prevention, it must be made accessible to everyone in need—a goal that remains out of reach for many. In 2023, the cost of Lenacapavir as an HIV treatment in the United States was $42,250 per patient per year (approximately 650 million Rupiahs!). Gilead Sci-ences has announced non-exclusive, royalty-free voluntary licensing agreements with six pharma-ceutical manufacturers to produce and sell generic Lenacapavir in 120 high-incidence, resource-limited countries. These agreements primarily cov-er low- and lower-middle-income countries. How-ever, middle-income countries, such as Brazil—where HIV infection rates remain high—are ex-cluded from these agreements. These countries will be forced to pay Gilead’s prices for Lenacapavir unless they successfully challenge unmerited patents on the drug.
UNAIDS has applauded Gilead’s announcement but strongly urges the company to extend voluntary licensing agreements to all low- and middle-income countries. They also welcomed Gilead’s statement of commitment to non-profit pricing but emphasized the urgency of specifying an actual affordable price. Research supported by the Make Medicines Affordable Campaign (MMA) es-timates that generic Lenacapavir could initially be mass-produced for $63–$93 per patient per year (PPPY), and with production volumes of 10 million, costs could fall further to $26–$40 PPPY. Efforts to oppose unmerited patents are underway, with MMA partners filing patent oppositions in Argen-tina, India, Indonesia, Thailand, and Vietnam.
Further research on Lenacapavir explores its use in combination with other drugs and the potential for yearly injections, fueling optimism for future advancements. Hopes are high for the years ahead; however, the core principle of UNAIDS, ‘Leave no one behind,’ must remain central to ensure equitable access and to envision a world free of HIV.
May I close this talk with: Happy New Year! Let’s move forward together and hope for a year filled with successful breakthroughs!
References
- Bekker, L.G., et al., 2024. Twice-yearly Lenacapavir or daily F/TAF for HIV prevention in cisgender women. New England Journal of Medicine.
- Cohen, J., 2024. The long shot. Science (New York, NY).
- Dvory-Sobol, H., et al., 2022. Lenacapavir: a first-in-class HIV-1 capsid inhibitor. Current Opinion in HIV and AIDS.
- Kelley, C.F., et al., 2024. Twice-yearly Lenacapavir for HIV prevention in men and gender-diverse per-sons. New England Journal of Medicine.
- Link, J.O., et al., 2020. Clinical targeting of HIV capsid protein with a long-acting small molecule. Nature.
- Neverette, N.C., et al., Lenacapavir: Playing the long game in the new era of antiretrovirals. Clinical Pharmacology & Therapeutics.
- Prather, et al., 2023. Lenacapavir: A first-in-class cap-sid inhibitor for the treatment of highly treatment-resistant HIV. American Journal of Health-System Pharmacy.
- Segal-Maurer, S., et al., 2022. Capsid inhibition with Lenacapavir in multidrug-resistant HIV-1 infection. New England Journal of Medicine.
- Wen, Z., et al., 2024. Treatment as the Best Prevention: Twice-yearly Lenacapavir, a game changer in ending the AIDS epidemic. Viruses.
- https://attheu.utah.edu/health-medicine/anti-hiv-drug-u-biochemist-helped-developed-named-breakthrough-of-the-year/
- https://makemedicinesaffordable.org/hiv-community-based-organizations-are-fighting-patent-monopolies-on-lenacapavir/
- https://www.gilead.com/news/news-details/2024/gilead-signs-royalty-free-voluntary-licensing-agreements-with-six-generic-manufacturers-to-increase-access-to-lenacapavir-for-hiv-prevention-in-high-incidence-resource-limited-countries
- https://www.npr.org/sections/goats-and-soda/2024/12/12/g-s1-37662/breakthrough-hiv-lenacapavir
- https://www.unaids.org/en/resources/presscentre/pressreleaseandstatementarchive/2024/october/20241002_gilead-lenacapavir
Most Commented